n 83-year-old female presented to the Casualty Department with lethargy and splenomegaly.
A FBC was performed with the following results:
Hb 89 g/L, WBC 140.8 x 109/L and Platelet count 23 x 109/L.
A differential white cell count showed an absolute neutrophilia and monocytosis. There was a left shift in the myeloid line with some dysplastic changes in both the neutrophils and the monocytes.
A diagnosis of chronic myelomonocytic leukaemia was made.
Myelodysplastic / myeloproliferative diseases:
Chronic myelomonocytic leukaemia

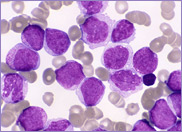
Peripheral blood film
Bone marrow
Chronic myelomonocytic leukaemia (CMML) is a clonal disorder closely resembling chronic myeloid leukaemia (CML). It is characterised by a persistent monocytosis of >1 x 109/L in the peripheral blood; absence of the Philadelphia chromosome and BCR/ABL fusion gene; dysplasia involving one or more cell lineages and < 20% blasts in the bone marrow. CMML occurs predominantly in patients over 50 years old. The peripheral blood is characterised by a monocytosis, usually in the range of 2-5 x 109/L. The percentage of monocytes is almost always >10% of the total white blood cell count. The monocytes are mature and often display abnormal nuclear morphology. Blasts and promonocytes account for approximately 20% of the white cells.
The total white cell count may be normal or slightly decreased.
A neutropenia or neutrophilia may be present. Neutrophil precursors usually comprise fewer than 10% of the total white cell count.
Some cases of CMML are associated with an eosinophilia. The eosinophil count is >1.5 x 109/L. Elevated eosinophil counts may be associated with tissue damage secondary to degranulation of the eosinophils.
Dysplasia is a feature of all three cell lineages occurring in both the peripheral blood and bone marrow. Dysgranulopoiesis: hypolobulated or abnormally lobulated nuclei with abnormal cytoplasmic granulation of the monocytes. Dyserythropoiesis: normocytic/macrocytic red cells.
Dysmegakaryopoiesis: thrombocytopenia with atypical large platelets.
CMML is divided into two categories according to the number of blasts in the peripheral blood and bone marrow. CMML-1: <5% blasts in the peripheral blood and <10% blasts in the bone marrow.
CMML-2: 5-19% blasts in the peripheral blood and 10-19% blasts in the bone marrow. More than 20% blasts in the peripheral blood or bone marrow are indicative of acute myeloid leukaemia rather than CMML.
The bone marrow in CMML is hypercellular with proportionally more promonocytes than monocytes. Often the myeloid hyperplasia of the marrow tends to mask the monocytosis.
Immunophenotype:
The peripheral blood and bone marrow cells express the typical myelomonocytic antigens, namely:
CD13 and CD33 (myeloid)
CD14, CD64 and CD68 (monocytoid)
Cytogenetics:
There is no Philadelphia chromosome in CMML.
Cytogenetic abnormalities occur in 20-40% of cases of CMML:
+8, -7del(7q) or del(20q).
The median survival of patients with CMML is 20-40 months. Progression to acute leukaemia occurs in approximately 15-30% of cases.