A 15 year old male presented with lethargy, pallor and bleeding from the gums. A full blood count was performed with the following results:
Hb 44 g/L, WCC 53.7 x 109/L and platelet count 12 x 109/L
The differential white cell count showed an absolute monocytosis of 10.7 x 109/L and a blast count of 22.5 x 109/L.
A bone marrow examination revealed a hypercellular marrow with 74% blast cells. The blasts had a round to convoluted nuclear appearance with a fine chromatin pattern and one or more nucleoli. The cytoplasm was basophilic and lacked granules. Morphologically, they resembled monoblasts.
Flow cytometry was performed on the marrow, which had the following immunophenotype:
CD13+/CD33+/CD34-/CD117+/HLA-DR+/TdT–/MPO+ (myeloid markers)
CD14–/CD64+/CD116+ (monocytoid markers)
The markers were suggestive of acute myeloid leukaemia with monocytic differentiation. As the blasts clearly resembled monoblasts morphologically, a combined esterase stain was performed. The blasts were positive with the a-naphthyl acetate esterase stain and negative with the AS-D chloroacetate esterase stain.
The overwhelming brown reaction, as seen below, confirmed the morphological diagnosis of acute monoblastic leukaemia.
Acute monoblastic leukaemia

Peripheral blood film
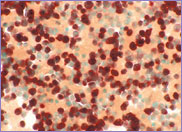
Bone marrow α-naphthyl acetate esterase stain
The WHO classification of acute monoblastic leukaemia, synonymous with M5a in the FAB classification, occurs at any age but most commonly occurs in young adults. The majority of cases present with bleeding gums secondary to gingival infiltration. Acute monoblastic leukaemia and acute monocytic leukaemia are myeloid leukaemias characterised by 80% or more cells of the monocytic lineage. In acute monoblastic leukaemia, at least 80% of the cells are monoblasts and in acute monocytic leukaemia, at least 80% of the cells are promonocytes and monocytes.
Monoblasts have rounded nuclei with a fine chromatin pattern and one or two prominent nucleoli. The cytoplasm is basophilic and lacks granules. Promonocytes show some differentiation in the maturation of the nucleus, which is indented and often contains a nucleolus. The cytoplasm is blue-grey and may contain a few fine azurophilic granules as well as vacuoles.
Monoblasts and promonocytes usually show -naphthyl acetate esterase positivity. In 10-20% of cases, the a-naphthyl acetate esterase stain is negative or weakly positive and immunophenotyping may be necessary to make a diagnosis.
The most common cytogenetic rearrangement associated with acute monoblastic leukaemia is t(8;16)(p11;p13). While the immunophenotype should show some markers characteristic of monocytic differentiation:
CD13+, CD33+, CD34–, CD117+ (myeloid markers)
CD4+, CD11b+, CD11e+, CD14+, CD36+, CD64+, CD68+ (monocytoid markers)
Many cases of acute monoblastic leukaemia will not express CD14, as it is a marker of monocytic differentiation.
Acute monoblastic and acute monocytic leukaemia usually have an aggressive clinical course. Prognosis is usually poor.
This particular case demonstrates the necessity to use all the available tools, namely, morphology, cytogenetics, immunophenotype and cytochemistry to make the correct diagnosis.